The lateral raise seems like such a simple exercise. How many variations can there possibly be? Well, the answer to that question, as I’ll soon show you, is “Plenty!” Since a recent study has revealed seven segments of the deltoid, not just three, and the ball and socket configuration of the glenohumeral joint allows more motion to occur at the shoulder than any other joint in the body (up to 16,000 positions for the arm), more areas can and should be stimulated (26, 21, 17).
Thus, it’s important to use many different angles when performing laterals if you really want to add some size and width to those delts! Let’s explore some options.
Fiber Type Distribution
There’s a low percentage of fast-twitch (FT) fibers in the medial deltoid, averaging 36% FT and 57% slow-twitch (25, 4), and according to Tesch and Larsson, “Fiber-type distribution pattern in present bodybuilders tends to resemble the muscle structural profile of endurance athletes. The bodybuilders did exhibit relatively high muscular endurance, which is consistent with the observed low percentage of high-glycolytic, fatigable FTb fibers.” (25)
Yet, paradoxically, the bipennate structure of the medial deltoid with five to seven tendons allows for powerful contractions. These strong, short fibers are less susceptible to intrinsic stretching and display their greatest strength at 90 degrees and are weakest at the upper and lower 15-degree range (6). It’s evident that the shoulders can withstand a high workload since they’re involved in almost every upper-body movement, and they’ll respond to a variety of rep ranges.
Abduction vs. Other Shoulder Movements
How does abduction (moving the arm away from the body) rate compared to the various other shoulder movements? About middle of the road. In general, adduction (toward the body) is higher than abduction torque (2:1), internal rotation is higher than external rotation torque (3:2), and extension is higher than flexion torque (5:4). Overall, according to Halder et al., “Adduction strength is highest, followed by extension, flexion, abduction, internal rotation, and external rotation.” (8) If you want to promote balance around the shoulder joint, consider the above-mentioned ratios. Remember, you’re only as strong as your weakest link!
Scapular Plane
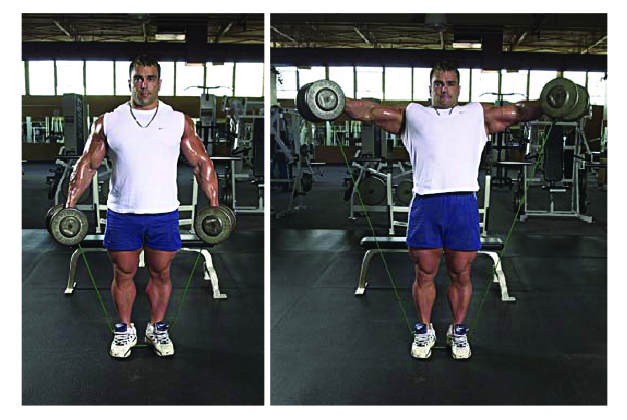
When performing a lateral raise, you should always concentrate on the elbows — raising them upward and outward until you reach ear level (2). Although there’s significantly less activity in the medial deltoid and supraspinatus during scapular plane elevation with the elbow bent compared with the elbow straight (due to a shorter lever arm), it’s a good idea to maintain a slight bend to relieve stress on the elbow joints (15).
Keep the wrists straight and firm and, as always, keep the chest up and out. It’s important to maintain a neutral spine and set the scapula through retraction. This transforms the upper back into a rigid, solid platform allowing greater deltoid isolation (3). Use a mirror to check for symmetry when performing a lateral raise with both arms. Actually, some authorities believe that the exercise should be done in this manner so that any compensatory motions can be easily detected (19).
Dale Buchberger, an ART practitioner
Not only do the deltoid and supraspinatus have a more direct line of pull in the scapular plane (1), there’s also increased

Okay fine, there may be some benefits to performing the lateral raise in the scapular plane, but really, how bad is the common method? Well, according to Rosenthal, “The lateral raise performed in the frontal plane with the arm extended reduces conformity of the joint surfaces, produces less than
Subacromial Impingement
Since the lateral raise is commonly performed with the palm facing down, the internal rotation of the glenohumeral joint can lead to rotator cuff impingement. Generally, the rotator cuff tendons move with minimal compression beneath the acromion when abducting the arm. However, if the arm is internally rotated excessively during elevation and/or raised beyond 90 degrees, the greater tuberosity of the humerus pinches the rotator cuff tendons and bursa against the acromion and repetitive aggravation can lead to inflammation and damage to these structures.
So what does this mean? Well, to minimize compression, don’t go beyond 90 degrees, or try doing laterals with the arms externally rotated where the thumbs are pointed toward the ceiling (3, 5, 17, 21). Never perform an exercise if it hurts, but with some modification – either to the plane of movement, grip position, or range of motion – you should be able to do it without pain.
Posterior Deltoids
Neglect any one of the deltoid heads and you’ll develop a muscle imbalance. Usually, the posterior (rear) deltoid is lacking — the classic “rounded shoulders” posture some bodybuilders get is a good example of this.
As Michael Gundill notes, “Bodybuilders have front delts that are on average five times bigger than sedentary people. Their lateral delts are three times bigger and their rear delts are only 10 to 15 percent bigger. That imbalance translates into supraspinatus tendon abnormalities and is a source of shoulder pain.” (7) To hit more posterior deltoid, keep your arm back in the frontal (coronal) plane and use an offset grip (more on that later), or you could bend over when performing lateral raises.
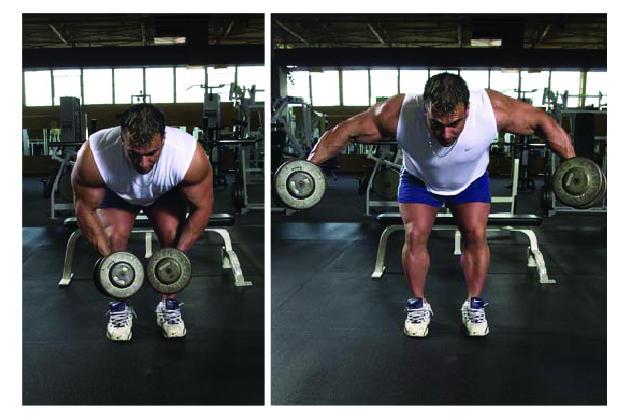
To reduce the stress to your lower back with this exercise, either rest your forehead on an incline bench, lie prone on a high bench (18), or perform the exercise unilaterally (i.e., one arm at a time) to allow the opposite hand to support the body (3).
Having a training partner touch the posterior delts while lifting will help focus attention and stimulate those muscles. Another tip offered by Beth and Oscar Rothenberg in their book Touch Training for Strength is to touch the elbows, then the ears, and ask the exerciser to draw an imaginary straight line between the two points as they lead the lift with their elbows (22).
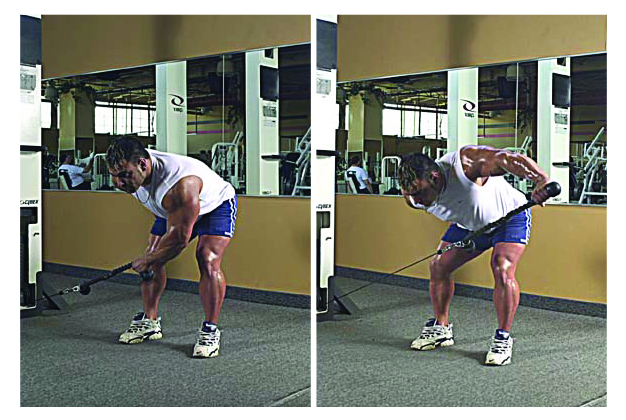
An excellent exercise for the posterior delt is the bent-over one-arm cable lateral raise (pronated grip) using a rope. Try it and you’ll see what I mean, but start with the lightest plate first.
Side-Lying vs. Lean-Away Laterals
McMahon et al., 1995 state that a larger contribution of force from the supraspinatus is required near the beginning of motion, whereas the middle deltoid is more important near the end of glenohumeral abduction in the scapular plane (12, 16).
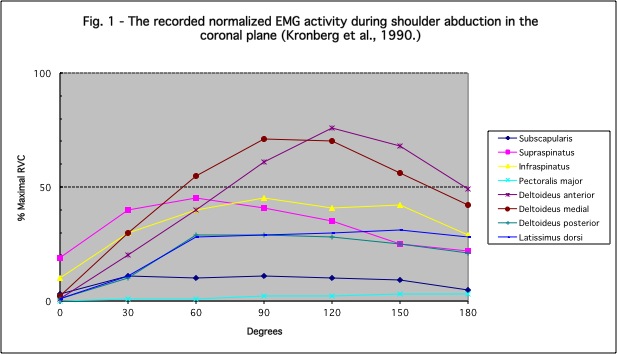
Therefore, side-lying on a bench or Swiss ball will effectively target the supraspinatus since the function of this rotator cuff muscle is to abduct the arm primarily during the first 15 to 30 degrees. This method of training also has important implications for physical rehabilitation of the rotator cuff since it displayed the greatest activation of shoulder muscles compared to other popular exercises while avoiding subacromial impingement (9).


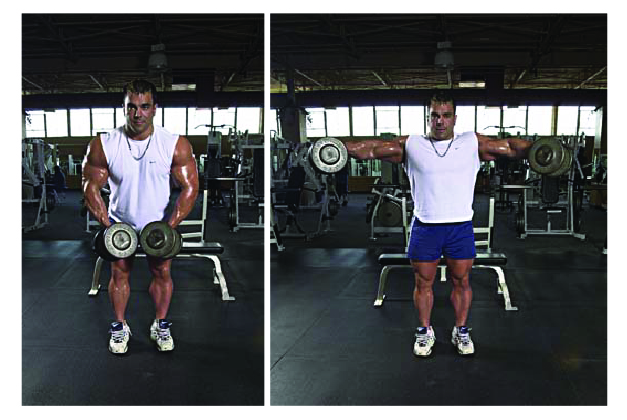
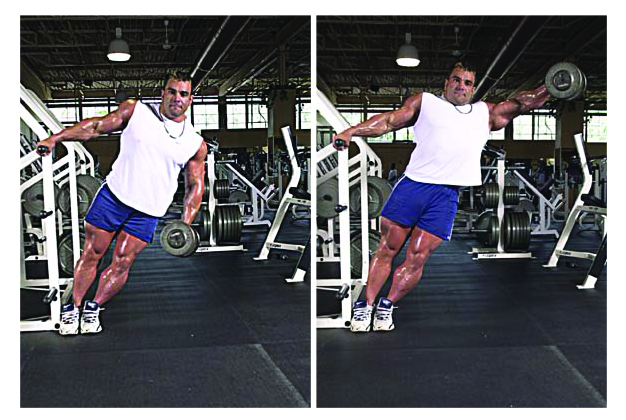
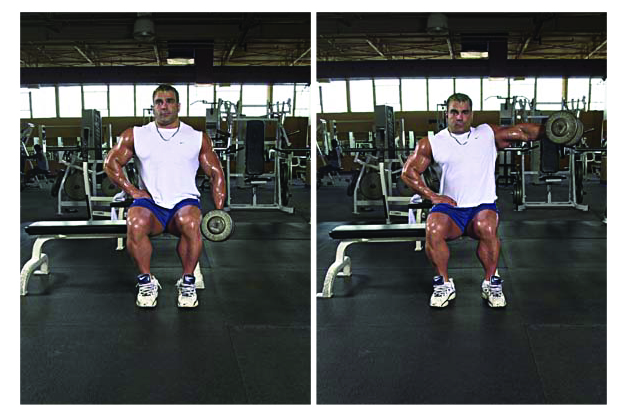
However, in order to truly target the fibers of the medial deltoid, use lean-away laterals where a greater overload is placed on the top of the movement.
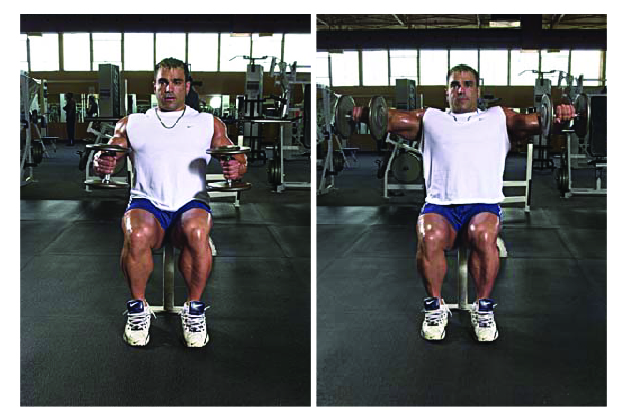
Standing or Seated?
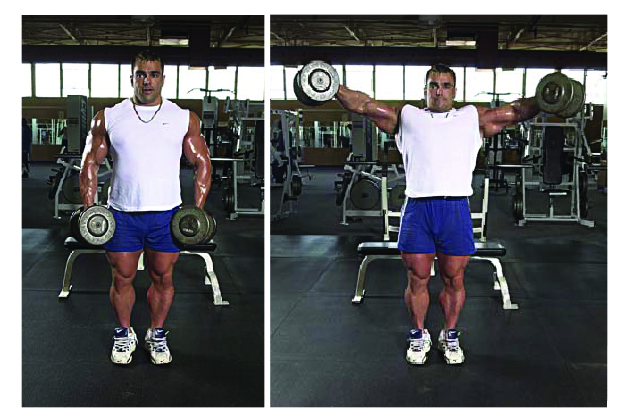
Dumbbell lateral raises can be performed standing or seated. Sitting when performing laterals will take the legs out of the movement and help you avoid cheating. However, you may wish to extend a set and the subsequent time under tension (TUT) by first sitting to isolate the delts and then, when you’re completely fatigued and can’t complete an additional concentric rep, standing to get help from your lower body to squeeze out another rep or two.
Full Range of Motion
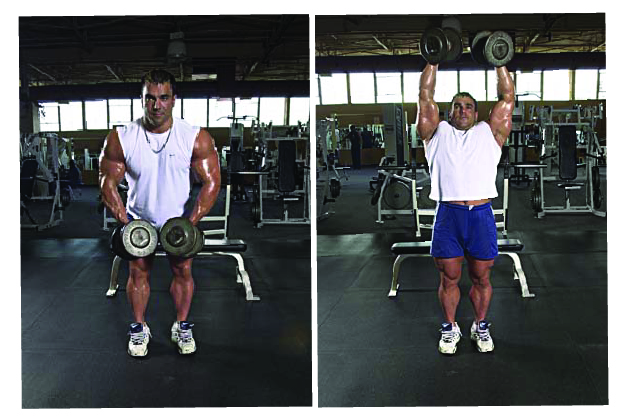
For regular dumbbell lateral raises, another option is to go to full range of motion (ROM) as recommended by Dr. Michael Yessis. As the arm passes 90 degrees, you must externally rotate the humerus to continue the motion so that the palms are facing each other at the bottom and top of the movement.
According to Yessis, “The deltoid is most active from the shoulder level position to the above-the-head position. Stopping at shoulder level as typically done in the lateral arm raise exercise limits flexibility in the shoulder joints and full muscular development.” (27) However, if rotation during full ROM laterals causes discomfort, only raise the arms to 90 degrees where they’re in a straight line with the shoulders (13). Keep in mind that the serratus anterior, rhomboids, levator scapula, and upper trapezius muscles really come into play above parallel (17).
Partial Range of Motion
As Ian King has noted previously in T-mag, going beyond 90 degrees of abduction (meaning above parallel to the ground) increases upper trap involvement. In fact, research shows that the upper trapezius fires maximally at 120 degrees of abduction (17).
Ian actually recommends a ROM of 45 degrees below and above parallel to target the medial delts. He advises to “intentionally and consciously aim to keep the upper trap as long as possible for as long a time as possible during all training reps.” (11) Of course, you’ll have to use a lighter weight with this technique, but it works! Try it.
Jettison Technique
To extend a set and further the TUT, use a dumbbell and rubber tubing simultaneously. When fatigue sets in and you can no longer complete another concentric repetition (in other words, the elbows don’t reach ear level), drop the tube handles and continue with only the dumbbells. I first learned of this method, called the Jettison Technique, in the book MASS! by Robert Kennedy and Dennis B. Weis. The technique can also be used on a number of different exercises, like arm curls and upright rows for example (10).
Methods to Alter Loading
• The motto “go heavier or go home” doesn’t apply to me since I work out in my basement, but it still holds true for those that go to the gym. (For me, the motto is “go heavier or go upstairs!”) Lateral raises are no different than any other exercise. Weight training is about progressive overload – you should strive to use heavier loads over time. Due to the poor leverage encountered in this movement, small-incremental loading (e.g., using PlateMate attachments) is warranted.
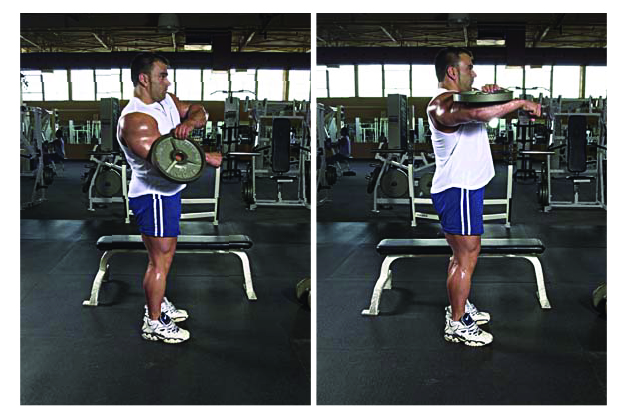
• Since the leverage is poor on lateral raises, bend the arm(s) to reduce the fulcrum (14, 23), which permits a slower tempo of execution since it makes the lift easier (20).
There’s a device called the Deltaforce which accommodates this action; however, you could save money by just supporting a weight plate on your upper arm or simply using dumbbells.
• An offset grip (thumb against plate) will recruit more posterior deltoid. To take this a step further, attach a PlateMate to the rear plate only (closest to your pinky).

• Body position will alter the line of pull. The standing lateral raise actually emphasizes the anterior deltoid. To challenge the middle deltoid, lean forward about 30 degrees (3). The more forward you
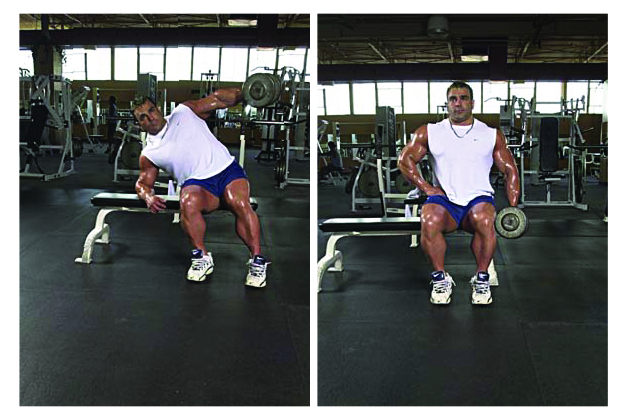
• Another interesting variation of body position is that proposed by exercise scientist Jerry Telle where the body moves from an upright position to a side-lying position during the eccentric action to maintain optimum tension on the delts (23, 24). At first, it may be difficult to execute smoothly, but after a few reps, you’ll get the hang of it.
Rotation of the arm will also influence the line of pull. For example, a slight internal rotation of the humerus so that the pinky is higher than the index finger throughout the ROM will increase the recruitment of the posterior deltoid. Keep in mind that excessive internal rotation will limit the ROM to 60 degrees or less, and shoulder impingement may occur. On the other hand, if shoulder external rotation is initiated early in the movement, the emphasis shifts to the anterior deltoid (3).
• Resistance tubing/bands will overload the top ROM and, as mentioned above, greater stress is placed on the medial deltoid.
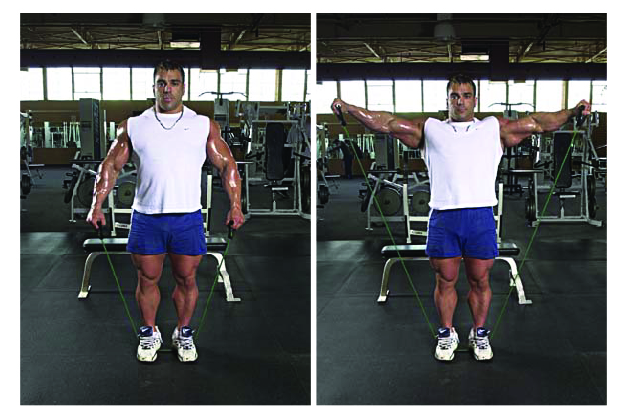
Cable resistance is even throughout the ROM, whereas dumbbells exert the greatest overload (or moment/torque) when the arm is exactly parallel to the ground.
Workouts
Okay, let’s put it all together now. Here are some sample programs:
Option A: Bilateral, Alter Lever Arm (Giant Set)
1) Seated Dumbbell Lateral Raise (straight arm on both concentric and eccentric)
Sets: 3-4 sets
Reps: 8-10 reps
Tempo: 3-0-3-0, no rest
2) Seated Dumbbell Lateral Raise (arm bent to 90 degrees on concentric, straight on eccentric)
Sets: 3-4
Reps: 8-10 reps
Tempo: 3-0-3-0, no rest
3) Seated Dumbbell Lateral Raise (arm bent to 90 degrees on both concentric and eccentric)
Sets: 3-4
Reps: 8-10
Tempo: 3-0-3-0, no rest
4) Standing Dumbbell Lateral Raise (arm bent to 90 degrees on both concentric and eccentric)
Sets: 3-4
Reps: as many reps as possible
Tempo: 1-0-1-0, 180 seconds rest
Option B: Unilateral, Alter Angle of Overload (Tri-Set)
1) Lean-Away Dumbbell Lateral Raise
Sets: 3-4
Reps: 10-12
Tempo: 2-0-1-2, no rest
2) Standing One-Arm Lateral Raise
Sets: 3-4
Reps: 10-12
Tempo: 2-0-1-2, no rest
3) Side-Lying Dumbbell Lateral Raise
Sets: 3-4
Reps: 10-12
Tempo: 2-0-1-2, 180 seconds rest
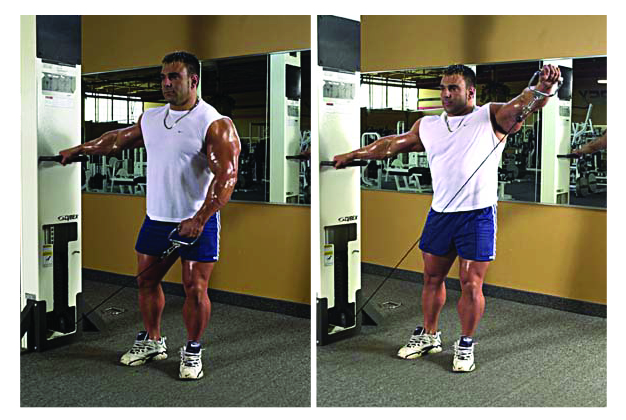
Option C: Unilateral, Induce Fatigue
One-Arm Cable Lateral Raise
Sets: 3-4 sets
Reps: 12-15
Tempo: 2-0-X-0 (alternating arms with no rest in between until all sets are complete — make sure to start with your weak side)
Conclusion
If you want to have trouble fitting through door frames, you need to do lateral raises. And if you want to get the most out of laterals, you need to do some “lateral thinking” and use many different variations of the exercise. Hopefully, I’ve given you enough ammo here to get you started.
References
1) Altchek DW, Levinson M. Shoulder injury in the throwing athlete. Phys Med Rehabil Clin N Am. 2000 Nov;11(4):745-54.
2) Baker, G. 1995: Exercises Of The Month. Strength and Conditioning: Vol. 17, No. 3, pp. 44—45.
3) Brooks, D. Shaping the Shoulder. http://www.ptonthenet.com/
4) Colling, R. 1997: Distribution of Human Muscle Fibre Type. Exercise Physiology 552. http://physiotherapy.curtin.edu.au/community/educational_resources/ ep552_97/fibretypedist.html
5) Durall, CJ, Manske RC, Davies GJ. 2001: Avoiding Shoulder Injury From Resistance Training. Strength and Conditioning Journal: Vol. 23, No. 5, pp. 10—18.
6) Goodmurphy, C. Pathology Workshop: Shoulder and Pelvic Girdle, 1998.
7) Gundill, M. Pressing Issues: Building better shoulders with overhead presses. Ironman. August 2002, pg. 42.
8) Halder AM, Itoi E, An KN. Anatomy and biomechanics of the shoulder. Orthop Clin North Am. 2000 Apr;31(2):159-76.
9) Horrigan JM, Shellock FG, Mink JH, Deutsch AL. Magnetic resonance imaging evaluation of muscle usage associated with three exercises for rotator cuff rehabilitation [Abstract]. Med Sci Sports Exerc 1999 Oct;31(10):1361-6
10) Kennedy, R, Weis, DB. MASS! Chicago, IL: Contemporary Books, Inc., 1986.
11) King, I. http://www.testosterone.net/articles/188metal.html
12) Kronberg M, Nemeth G, Brostrom LA. Muscle activity and coordination in the normal shoulder. An electromyographic study. Clin Orthop. 1990 Aug;(257):76-85.
13) Kurland, H. 1981: Training the Shoulder for Baseball. National Strength Coaches Association Journal: Vol. 3, No. 5, pp. 28—31.
14) Lander, J, Rutland, R. How Much Weight Are You Really Lifting? http://www.cybexintl.com/education/perf_training/how_much_weight.html
15) McCann PD, Wootten ME, Kadaba MP, Bigliani LU. A kinematic and electromyographic study of shoulder rehabilitation exercises. Clin Orthop. 1993 Mar;(288):179-88.
16) McMahon PJ, Debski RE, Thompson WO, Warner JJ, Fu FH, Woo SL. Shoulder muscle forces and tendon excursions during glenohumeral abduction in the scapular plane [Abstract]. J Shoulder Elbow Surg 1995 May-Jun;4(3):199-208
17) Moseley JB Jr, Jobe FW, Pink M, Perry J, Tibone J. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 1992 Mar-Apr;20(2):128-34.
18) Pierce, KC. 1998: Exercises Of The Month: Bent-Over Lateral Raise and Jerk From Rack. Strength and Conditioning: Vol. 20, No. 5, pp. 42—53.
19) Pink MM, Tibone JE. The painful shoulder in the swimming athlete. Orthop Clin North Am. 2000 Apr;31(2):247-61.
20) Poliquin, C. The Poliquin Principles. The Dayton Writers Group, 1997.
21) Rosenthal, MD. 1997: Shoulder Savers: Alterations of Traditional Exercises. Strength and Conditioning: Vol. 19, No. 2, pp. 7—10.
22) Rothenberg, B, Rothenberg, O. Touch Training for Strength. Champaign, IL: Human Kinetics, 1995.
23) Telle, J. Beyond 2001 – The Next Real Step. New approaches to scientific training for the advanced bodybuilder (Coaches Edition.) Denver, CO., 1998.
24) Telle, J. Tellekinetics — A New Way to Train Shoulders. http://www.testosterone.net/html/50telle.html
25) Tesch PA, Larsson L. Muscle hypertrophy in bodybuilders. Eur J Appl Physiol Occup Physiol. 1982;49(3):301-6.
26) Wickham JB, Brown JM. Muscles within muscles: the neuromotor control of intra-muscular segments [Abstract]. Eur J Appl Physiol Occup Physiol. 1998 Aug;78(3):219-25
27) Yessis, M. http://www.dryessis.com/html/tips.html


